We extend the mandates that do nothing and we ignore the mandates that would work. That’s just the way “science” works in today’s world. Get used to it.
By Steve Kirsch
Overview
- Mask mandates don’t work at all, so they are being extended on public transportation.
- There are two mandates, based on science, that are effective: 1) if you are sick, stay home until your symptoms resolve and 2) if you exhibit COVID symptoms, start a proven early treatment protocol immediately. Unfortunately for us, no public health official is ever going to mandate either measure. It would make too much sense to do that.
The mandate that does nothing other than piss people off is extended for a month
Mask mandates on public transport have been extended for another month even though they don’t work

The CDC has directed the TSA to extend the public transportation mask mandate for another 30 days until April 18 according to this CNN article.
Here is the science behind this decision, a list of studies showing that transmission on public transportation is a major component of viral spread and showing that face masks effectively mediate that risk:
< this space intentionally left blank >
In fact, if you have to be indoors, being on board a commercial jet is probably one of the safest places you can be because the recycled air is filtered with HEPA filters (shown below), the cabin air is recycled every 3 minutes, and there is a high portion of outside air mixed in the filtered inside air.
What does the science say about air quality on planes? Here you go:
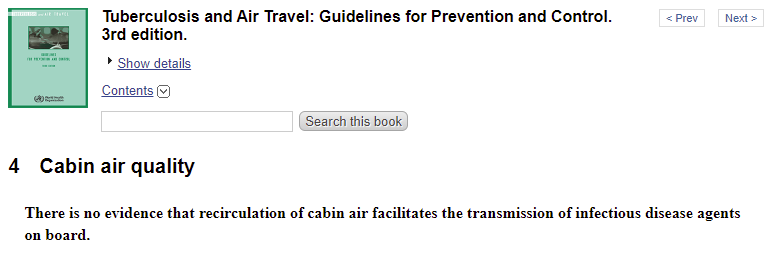
If you are sitting very close to an infected person who is symptomatic, you may be at risk. The paper above acknowledged that risk. But that risk only applies if the person is right next to you.
And there is no scientific evidence whatsoever that wearing a mask reduces your risk of getting infected in such a case since all the randomized trials on masks and COVID have shown masks make no difference.
If anything, this has been a giant science experiment over the last 2 years that proved that mitigation strategies on board were completely unnecessary since they made no difference.
Nobody complained that “wow, even with the mask mandate, transmission on public transportation has been unacceptable.”
So masks “worked” even though they did nothing. It was pure placebo effect and it resulted in nobody having any fears about getting sick on the plane.
Have you seen a documented case of COVID transmission on public transport after the mask mandates started? I haven’t. There wouldn’t be because it would destroy the narrative that masks work.
So we know two things:
- Masks do nothing to stop the spread of COVID
- Masks “work” effectively on public transit because they aren’t stopping any public transit anywhere due to COVID spread on public transit.
In short, we’ve proved that no mitigation strategies were ever required on public transit to reduce the spread of disease.
It was all political theater to give people the impression that they were “safe” if they used public transit. It worked brilliantly as few people ever figured it out.
The two mandates that work
Nobody is going to implement the two mandates that work. I’m mentioning them here just for reference to prove that, yeah, people did propose stuff that works, but were ignored:
- If you are sick, stay home until your symptoms resolve.
Asymptomatic spread is largely non-existent. That’s what the science says. So what do we do? We set arbitrary time limits for quarantines instead of taking a scientific, risk-based approach. - If you have COVID, start a proven early treatment protocol using known safe, repurposed drugs and supplements such as the Fareed-Tyson protocol. At a very minimum, do a nasal rinse for 7 days.If you do this early in the disease, it is extremely unlikely you will need to be hospitalized or die.
Even just a nasal rinse with povidone iodine in an isotonic saline solution diluted to 0.1% concentration for 7 days is highly effective
Even something simple and low cost such as nasal irrigation with a 0.1% povidone iodine solution has been shown to be remarkably effective.
The CDC is simply never going to let the public know about this.
That was not a typo. Previous studies used a 1% solution, but this paper used a 100X dilution of the 10% solution you can buy at most pharmacies for less than $10. You can buy it on Amazon for just $7. The bottles are good for 100 rinses, and the study had people do 2 rinses a day for 14 days, so each $7 bottle lasts for 4 COVID infections, so we are looking at a cost of less than $2 to treat a COVID infection.
You just mix 240 ml of purified water, 1/2 tsp of non-iodized salt, and 2.4 ml of the 10% povidone iodine solution. Then use a NeilMed squeeze bottle or Neti pot to administer. It’s very fast and easy.
Note that they never did any dosing studies and the .1% was just as effective as the 1% solution, so it’s likely that even the 2.4 ml solution is overkill. The mixture is fairly dark even at the 0.1% concentration and it can permanently stain items that are exposed to it.
The study had participants rinse twice a day for 14 days.
From a mechanism of action point of view, that 14-day recommendation was likely overkill since the viral replication phase is done after 7 days. This is one of my biggest complaints with studies is that they never do a rapid study phase of the trial (unblinded) to find the best dose before they run the trial.
The bottom line is that practically speaking, you’re looking at a cost of less than $1 per infection.
No doctor visit or prescription is required.
I predict that what will happen after this becomes more well know is that the FDA will make noise about making povidone iodine suddenly available only by prescription just like they did with NAC after it was shown to be effective in mitigating COVID symptoms.
That’s just the way the system works: any time you find something that works for COVID that isn’t from big pharma, the FDA or NIH finds a way to put up roadblocks or create fear, uncertainty, and doubt (FUD) to using it like they did with ivermectin, fluvoxamine, NAC, etc.
Aspirin and vitamin D are two other very safe and easy mitigation strategies. Again, no uptake from any public health official in the US.
Summary
We extend the mitigation strategies that don’t work and we ignore the mitigation strategies that do work. This allows politicians to extend the state of emergency so they can keep control over what we do.
Those who speak out against this are ignored and marginalized. I fear this is just going to get worse over time.