Can We Please Stop Demonizing the “Unvaccinated?”
By Debbie Lerman ( Brownstone Institute)
When the Covid vaccines first came out, I thought everyone should get at least one shot. My belief was based on evidence that the vaccines significantly lowered the risk of bad outcomes (hospitalization/death), and on what was thought at the time to be the vaccines’ ability to prevent infection and transmission.
For those in high-risk groups, like older people with underlying conditions, I thought the vaccine was important because it lowered their relatively high risk of dying from the virus. For young, healthier people I thought it was important to lower the risk of infection and transmission in order to protect more vulnerable populations.
That was in late 2020 and early 2021. We now know a lot more about the vaccines and about acquired immunity. Most importantly, we know that while vaccines give good but waning protection from bad outcomes, they do not prevent a person from getting a Covid infection or transmitting the virus to another person. We also know that having had Covid gives you at least as much protection from bad outcomes as the vaccine does.
This is crucial information that must be incorporated into how we view vaccines and how we view each other.
Unfortunately, when I talk to my friends who have been in a so-called “liberal” bubble for the past two years, they are shocked to hear that an unvaccinated person poses as much, or as little, risk to others as we – the triple vaxxed! – do. They just have this feeling that someone who’s unvaccinated is dangerous to them, or to society, in some way.
I understand where their fear and misunderstanding come from. First, of course, is the ocean of hysteria and misinformation they’ve been swimming in for the past two years. Second is the original (and in some places ongoing) vaccine campaign that emphasizes the importance of protecting not just oneself but others. Third is the experience we’ve had with other vaccines that have been able to eradicate or at least very radically reduce the prevalence of serious diseases like polio.
Given all that baggage, I’m finding it very hard to change people’s minds. Yet I persist.
Other than a simple pursuit of scientific data and truth, I believe it’s crucial to disabuse my friends and neighbors of the unfounded biases they harbor against “the unvaccinated” because that is turning into a label used to unnecessarily and unjustly marginalize a whole group of people. Like “the untouchables” or “the undocumented” this type of label contains a pejorative assumption about the members of the group that, in turn, justifies negative treatment of them.
In my world of the liberal coastal elites, the negative treatment of “the unvaccinated” manifests itself mostly in unjust exclusion from the places I used to view as the most inclusive, enlightened and welcoming: performing arts venues, community arts organizations, colleges and universities.
In my campaign to stop this negative treatment, I hereby beseech the leaders of such organizations and anyone else who can speak out on such matters to stop making fear-based decisions and refrain from using judgment-laden labels to justify such decisions.
Vaccine mandates have no public health benefit, which is why they are not recommended by any global, national or local public health bodies (WHO, CDC, state and local health commissions, etc.).
Therefore, any institution that still has such mandates is going against the recommendations of public health experts to unjustly discriminate against a very large group of people. Another important point is that, in the US, “the unvaccinated” include a disproportionate number of people of color and young people (see CDC data), which means the bias against this group overlaps with biases against traditionally marginalized populations.
Here’s what I want my friends, neighbors, arts/education leaders and anyone interested in truth and justice to do:
1) Let’s stop using the term “the unvaccinated” as a blanket putdown. Many people from many different demographic, scientific, cultural and religious groups have decided for whatever reason not to get the Covid vaccine and/or not to get boosted. Many of them have already had and recovered from Covid. None of them poses more danger to others than a vaccinated person does.
2) Anyone at an institution that still has vaccine mandates should come out strongly and forcefully against the mandates and explain why they are not just unnecessary, but unjust.
3) We should all educate ourselves about the ever-evolving state of the SARS-CoV-2 virus, the vaccines, and public health, to make sure we are not basing policies on outdated guidelines or unsupported assumptions.
Thankfully we are moving away from many of the deeply misguided, terribly damaging Covid policies that have plagued us (pun intended) for the last two years. Let us now work together to get rid of this last vestige of scientifically ignorant, panic-induced groupthink.
The Global March of Folly
By ( Spiked Online)
Throughout the pandemic, the media have eagerly compared Covid statistics between different countries. But such comparisons are often deceptive.
Take, for example, the use of Covid case counts. These depend not only on the number of people infected but also on the amount of testing performed. While useful for evaluating whether cases are increasing or decreasing within a particular country, they are deceptive when comparing countries. If we truly wanted to know, it would be easy, through random seroprevalence surveys that measure the proportion of people with antibodies. But not all governments have been eager to conduct these surveys, while some scientists have even got into trouble for doing them.
Comparing Covid death tolls between countries, as many journalists have done, is equally problematic. A Covid death is defined differently in different countries, with varying testing thresholds and a different maximum number of days required between a positive test and death. Therefore, countries vary in the proportion of reported Covid deaths that, firstly, are genuinely due to Covid, secondly, have Covid as a contributing factor but not as the main cause, and, thirdly, that show whether an individual died with rather than from Covid.
This confusion can lead to an over-reporting of Covid deaths. If we truly wanted to know, it would be easy. We could randomly select some reported deaths and evaluate their medical charts. Surprisingly few such studies have been performed.
Other countries have under-reported Covid mortality. For example, Nicaragua has reported very few Covid deaths. However, from reports that carpenters were working overtime to fulfill the burgeoning demand for wooden burial coffins in 2020, we certainly know that large numbers of people were dying from Covid there.
The media have also been tripped up by several significant variables. For example, the pandemic arrived and surged at different times in different countries, and even within countries – as you would expect from any pandemic. During the first wave in 2020, some countries were praised for their strict lockdowns and low Covid mortality, but subsequent waves hit some of them so badly that they now have among the highest mortality numbers in the world.
Covid is also seasonal. This means that it follows different seasonal patterns in different regions. This fact also tripped up journalists. In 2021, many journalists (often New York-based) blamed the seasonal summer wave in the southern United States on Covid policies. But when the subsequent winter wave arrived in the northern US, it was clear to all that it was a seasonal effect.
Extreme Covid restrictions, such as those imposed by Australia, Hong Kong and New Zealand, certainly kept the virus at bay for a while. But that just postponed the inevitable. All countries have to work their way through the pandemic sooner or later.
Moreover, the focus on Covid cases, death counts and so on, ignores the collateral public-health damage from Covid restrictions. These have contributed to deaths from other diseases, and such deaths are just as tragic as Covid deaths. A basic public-health principle is that one should never focus on one single disease but consider public health as a whole. Even if the lockdowns reduced Covid mortality, for which there is scant evidence, one must also consider the harm that the lockdowns caused on other health conditions such as worsening cardiovascular-disease outcomes, missed cancer screening and treatment, lower childhood-vaccination rates, and deteriorating mental health.
Given all this, how should we compare countries’ handling of the pandemic? While not perfect, the best way is to compare excess mortality; that is, the observed total number of deaths during the pandemic minus the average number of deaths observed during the years before the pandemic. Since the pandemic is not yet over, we do not have the full picture yet. Nevertheless, a recent article in the Lancetpresents excess deaths for 2020-2021 for almost every country in the world. The map below shows the results:
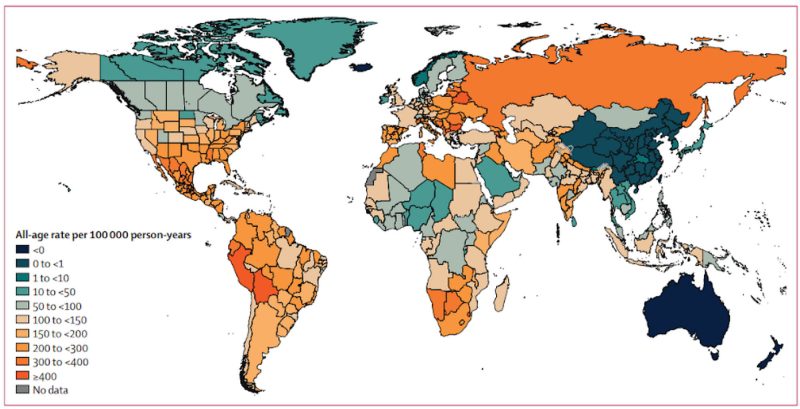
What can we learn from these data? How did three main pandemic strategies compare: (a) a do-nothing, let-it-rip approach; (b) focused protection of high-risk older people with only limited restrictions on others, and (c) general lockdowns and restrictions on all age groups?
Belarus and Nicaragua did little to protect older people and they imposed very few Covid restrictions. They also report among the lowest Covid mortality numbers. From the excess-mortality data, it is clear that they did not escape the pandemic. Nicaragua had 274 excess deaths per 100,000 population, which is precisely the same as the regional average. Belarus had 483 excess deaths per 100,000, higher than the average for either Eastern Europe (345) or Central Europe (316).
In Western Europe, the Scandinavian countries had the lightest Covid restrictions while they tried to protect their older high-risk population. Sweden was heavily criticised for this by the international media. The Guardian, for instance, reported in 2020 that life in Sweden felt ‘surreal’, with ‘couples stroll[ing] arm in arm in the spring sunshine’. Many journalists, politicians and scientists expected that the lighter Scandinavian touch would lead to disaster. That did not happen. Sweden has among the lowest reported Covid mortality numbers in Europe. Of the European countries with more than one million people, Denmark (94), Finland (81), Norway (7), and Sweden (91) are four of only six countries with excess mortality less than 100 per 100,000 inhabitants, the other two being Ireland (12) and Switzerland (93).
What about the UK, with its more heavy-handed Covid restrictions? Compared to the Western European average of 140 excess deaths per 100,000, England had 126, Scotland 131, Wales 135, and Northern Ireland 132.
In the US, South Dakota imposed few Covid restrictions, while Florida tried to protect older people without too many restrictions on the general population. Did that result in the predicted disaster? No. Compared to the national average of 179 excess deaths per 100,000, Florida had 212 while South Dakota had 156.
Countries in Sub-Saharan Africa report the lowest Covid mortality globally, with seven deaths per 100,000, but their excess mortality is 102 deaths per 100,000. Without age-stratified numbers, we do not know how much of this difference is due to the under-reporting of Covid deaths as opposed to the harsh lockdowns that caused malnutrition and starvation among the poor.
The countries with the highest excess mortality are Bolivia (735), Bulgaria (647), Eswatini (635), North Macedonia (583), Lesotho (563), and Peru (529), with no other countries topping 500 excess deaths per 100,000. According to the Oxford Stringency Index, Peru has endured some of the world’s harshest Covid restrictions while those in Bulgaria, Eswatini and Lesotho were closer to the average. Bolivia had very harsh restrictions in 2020, but not in 2021.
Though excess-mortality data should still be treated with caution, they do show that the few places that rejected draconian Covid restrictions did not see the catastrophic death counts that some had predicted.
The pandemic is not over, and with different seasonal patterns in different regions and different levels of population immunity, some countries have not yet seen the worst. For example, 40 per cent of all reported Covid deaths in Denmark occurred during the first 80 days of 2022. Denmark is not as extreme a case as Hong Kong, where 97 per cent of all reported Covid deaths have been in 2022.
The biggest weakness of excess-mortality statistics is that while they count Covid deaths, they do not fully capture the deaths, not to mention the collateral public-health damage, that come from Covid restrictions themselves. Missed cancer screenings and treatments do not lead to immediate deaths, but a woman who missed her cervical cancer screening may now die three or four years from now instead of living another 15 or 20 years. The mortality statistics do not reflect non-fatal collateral damage such as increasing mental-health problems or missed educational opportunities, either. Those harms need to be tallied and addressed in the years to come.
Politicians argued that the draconian lockdowns were needed to protect lives. From the excess-mortality data, we now know they were not. Instead, they have contributed to the enormous collateral damage that we will have to live with for many years to come. It is tragic.
In her classic book, The March of Folly, historian Barbara Tuchman describes how nations sometimes pursue actions contrary to their interests. She starts with Troy and the Trojan horse and ends with the US and the Vietnam War. By ignoring basic, long-standing principles of public health during the pandemic, most nations marched down the path of folly together. The leaders of those nations will be fine, except for some early retirements. The devastation on children, the poor, the working class and the middle class, on the other hand, will take decades to repair.
The New Normal
Lockdowns were not just an untested public health measure. They were a new paradigm of governance.
From the lepers in the Old Testament to the Plague of Justinian in Ancient Rome to the 1918 Spanish Flu pandemic, covid represents the first time ever in the history of managing pandemics that we quarantined healthy populations. While the ancients did not understand the mechanisms of infectious disease—they knew nothing of viruses and bacteria—they nevertheless figured out many ways to mitigate the spread of contagion during epidemics. These time-tested measures ranged from quarantining the sick to deploying those with natural immunity, who had recovered from illness, to care for them.
Lockdowns were never part of conventional public health measures. In 1968 1-4 million people died in the H2N3 influenza pandemic; businesses and schools never closed, and large events were not cancelled. One thing we never did until 2020 was lockdown entire populations. And we did not do this because it does not work. In 2020 we had no empirical evidence that it would work, only flawed mathematical models whose predications were not just slightly off, but wildly off by several orders of magnitude.
These devastating economic consequences were not the only major societal shifts ushered in by lockdowns. Our ruling class saw in Covid an opportunity to radically revolutionize society: recall how the phrase “the new normal” emerged almost immediately in the first weeks of the pandemic. In the first month Anthony Fauci made the absurd suggestion that perhaps never again would we go back to shaking hands. Never again?
What emerged during lockdowns was not just a novel and untested method of trying to control a pandemic by quarantining healthy people. If we view lockdowns outside of the immediate context in which they supposedly functioned in early 2020, their real meaning comes into focus. Changes ushered during lockdowns were signs of a broader social and political experiment “in which a new paradigm of governance over people and things is at play,” as described by Italian philosopher Giorgio Agamben. This new paradigm began to emerge in the wake of September 11, 2001.
The basic features were already sketched back in 2013 in a book by Patrick Zilberman, professor of the history of health in Paris, called “Microbial Storms,” (Tempêtes microbiennes, Gallimard 2013). Zilberman’s description was remarkably predictive of what emerged during the first year of the pandemic. He showed that biomedical security, which was previously a marginal part of political life and international relations, had assumed a central place in political strategies and calculations in recent years. Already in 2005, for example, the WHO grossly over-predicted that the bird flu (avian influenza) would kill 2 to 50 million people. To prevent this impending disaster, WHO made recommendations that no nation prepared to accept at the time—including population-wide lockdowns. Based upon these trends, Zylberman predicted that “sanitary terror” would be used as an instrument of governance.
Even earlier, in 2001, Richard Hatchett, who served as a member of George W. Bush’s National Security Council, was already recommending obligatory confinement of the entire population. Dr. Hatchett now directs the Coalition for Epidemic Preparedness Innovations (CEPI), an influential entity coordinating global vaccine investment in close collaboration with the pharmaceutical industry. CEPI is a brainchild of the World Economic Forum (WEF) in conjunction with the Bill and Melinda Gates Foundation. Like many others, Hatchett regards the fight against Covid-19 as a “war,” on the analogy to the war on terror. I confess that I took up the martial rhetoric early in the pandemic: in a March 2020 piece entitled, “Battlefield Promotions,” I issued a call to action encouraging medical students to stay involved in the covid fight after they had been sent home. While the piece had some merit, I now regret my deployment of this military metaphor, which was misguided.
A kind of overbearing medical terror was deemed necessary to deal with worst-case scenarios, whether for naturally occurring pandemics or biological weapons. Agamben summarizes the political characteristics of the emerging biosecurity paradigm:
1) measures were formulated based on possible risk in a hypothetical scenario, with data presented to promote behavior permitting management of an extreme situation; 2) “worst case” logic was adopted as a key element of political rationality; 3) a systematic organization of the entire body of citizens was required to reinforce adhesion to the institutions of government as much as possible. The intended result was a sort of super civic spirit, with imposed obligations presented as demonstrations of altruism. Under such control, citizens no longer have a right to health safety; instead, health is imposed on them as a legal obligation (biosecurity).
This is precisely the pandemic strategy we adopted in 2020. Lockdowns were formulated based on discredited worst-case-scenario modeling from the Imperial College London, which predicted 2.2 million deaths in the U.S. As a consequence, the entire body of citizens, as a manifestation of civic spirit, gave up freedoms and rights that were not relinquished even by the citizens of London during the bombing of the city in World War II (London adopted curfews but never locked down). The imposition of health as a legal obligation was accepted with little resistance. Even now, for many citizens it seems not to matter that these impositions utterly failed to deliver the public health outcomes that were promised.
The full significance of what transpired over the last two years may have escaped our attention. Perhaps without realizing it, we just lived through the design and implementation of a new political paradigm—a system that was for more effective at controlling the population than anything previously done by Western nations. Under this novel biomedical security model, “the total cessation of every form of political activity and social relationship [became] the ultimate act of civic participation.” Neither the pre-war Fascist government in Italy, nor the communist nations of the east, ever dreamed of implementing such restrictions. Social distancing became not just a public health practice but a political model and the new paradigm for social interactions, “with a digital matrix replacing human interaction, which by definition from now on will be regarded as fundamentally suspicious and politically ‘contagious’,” in Agamben’s words.
For the sake of health and human flourishing, this new normal should never be normalized.