1. Introduction
Readers of the D4CE website will be familiar with the atrocious safety record of the mRNA COVID vaccines produced by Pfizer and Moderna [1]. One striking feature is that adverse events occur not only after the first injection but also after every booster shot. In this short article, we will examine the reason for this observation. Other aspects of mRNA vaccine toxicity have been discussed by the D4CE before [2,3].
2. How the mRNA COVID vaccines work
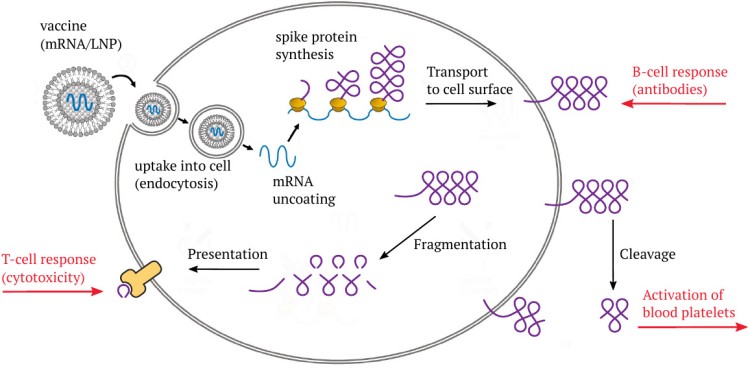
The Pfizer and Moderna mRNA vaccines consist of a synthetic messenger RNA (mRNA) that encodes the SARS-CoV-2 “spike protein,” which is normally found on the surface of the coronavirus particles. This mRNA is coated with a mixture of synthetic lipids—fat-like molecules—that protect it from degradation during transport within the body, and which also facilitate its uptake into the target cells through endocytosis.
After the vaccine particle has entered a cell, the lipids are stripped off, and the mRNA is released into the cytosol (the intracellular fluid). The mRNA then binds to ribosomes—the cell’s little protein factories—and directs them to synthesize the actual spike protein molecules. Most of the spike protein molecules will then be transported to the cell surface.
Sooner or later, cells that express this protein, or the remnants of such cells, will reach the organizational centers of the immune system in the lymphatic organs. The spike protein will then be recognized by various types of immune cells, including B-lymphocytes (B-cells), which will begin to make antibodies to it.
Furthermore, as with any protein that is synthesized within the cell, a small number of molecules will undergo fragmentation, and the fragments will be presented on the cell surface in association with specific (HLA-) carrier proteins. The purpose of this mechanism is immune surveillance: as soon as fragments show up of some protein which the immune system does not recognize as “self,” that is, as belonging to the human body, an immune response will be mounted against any cells that produce it. This response will result in the formation of cytotoxic T-lymphocytes (T-killer cells) that attack and destroy the cells which present those antigen fragments.
The cytotoxic activity of the T-killer cells will be augmented by several other immune effector mechanisms that are initiated by the antibodies. If this combined immune attack happens to the cells that line the blood vessels—the endothelial cells—the resulting lesion may cause blood clotting. Stroke, heart attacks, and thromboses must be expected, and many such cases have indeed been reported as adverse events after vaccination with Pfizer’s and Moderna’s COVID-19 mRNA vaccines (as well as with the adenovirus-based vaccines produced by AstraZeneca and Johnson & Johnson).
These immunological mechanisms must be expected to operate with any other mRNA-encoded viral antigens. In the case of COVID19 vaccines, there is a second, unique pathway that connects expression of the spike protein to vascular disturbances. A centrally important part of the spike protein (the S1 fragment) can be cleaved off and released from the cell. The S1 fragment can then bind to blood platelets (thrombocytes) and to endothelial cells at remote sites, effecting their activation. This second pathway of triggering vessel damage and blood clots is specific for the SARS-CoV-2 spike protein.
3. How the immune system deals with natural viruses (or live vaccines)
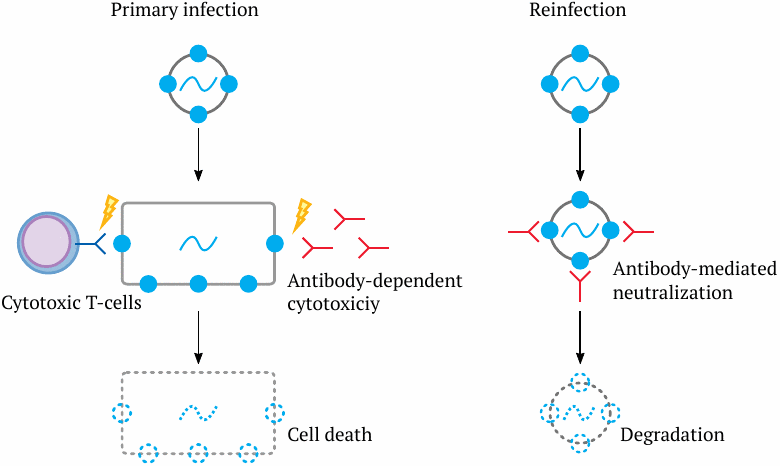
The immune system’s reaction to the expression of an mRNA vaccine is rather similar to the response of an immunologically naive host to the first infection with a new virus. In this situation, there is nothing to prevent the virus from entering a cell. Once inside the cell, the viral genome will direct the expression of viral proteins, which again will appear on the cell surface—some of them in intact form, and all of them as fragments, as discussed above. Accordingly, cytotoxic T-cells and antibody-dependent effector mechanisms will jointly attack the infected cell and kill it off. The death of infected cells on a large enough scale will cause inflammation and clinical disease.
Now, what happens if we are infected with the same virus again? In this case, we will already have antibodies to it, and these will bind many of the virus particles and prevent them from entering our body cells. Instead, the antibody-bound virus particles will be taken up by phagocytes and undergo destruction.1
Essentially the same kind of immune response is triggered by live virus vaccines, such as for example the measles vaccine. The difference is that the virus strain used for vaccination has been “attenuated” so as to not cause significant disease even after the first infection.
4. How the immune system reacts to mRNA vaccines
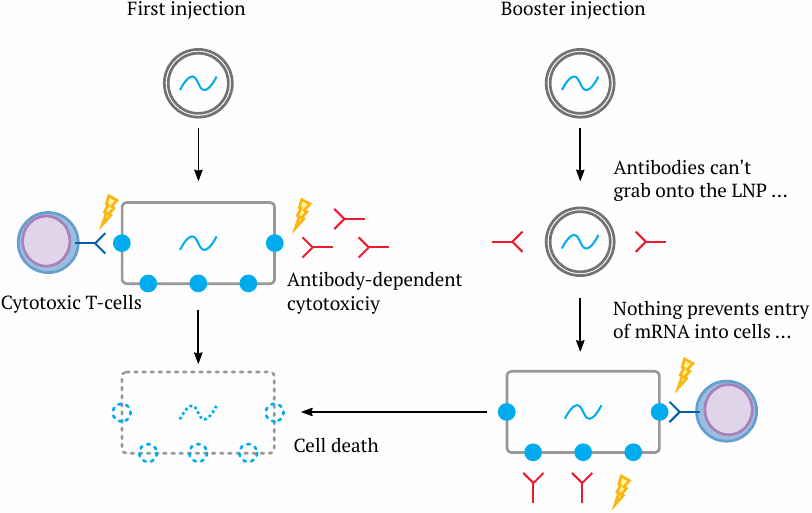
As noted above, the first injection of an mRNA vaccine will set off a sequence of events not unlike the one we see in a viral infection—the mRNA will initiate the synthesis of the protein antigen it encodes, and the immune system will generate antibodies and cytotoxic T-cells directed against that antigen. Together, these will cause the death of the cell.
What happens if we administer a booster injection of the same vaccine? Antibodies to the antigen in question will now be present. However, unlike a proper virus, the vaccine particles contain only the mRNA blueprint, but no protein copies of the antigen. Thus, the antibodies will be unable to recognize and grab onto the vaccine particles. Accordingly, nothing can prevent the mRNA from entering the body cells and expressing the antigen, and the immune system from attacking those cells. What is is more, the immune system will already be primed to attack faster and more forcefully.
The same will happen not just after the second injection, but after each and every booster injection. Similarly, individuals who have already had COVID-19 and thus have acquired natural immunity are at increased risk of adverse events even after the first mRNA vaccine injection [4,5]. You will be able to draw your own conclusions regarding the wisdom of sentencing the people, in many jurisdictions including even those with documented natural immunity, to a seemingly endless series of mRNA booster shots against COVID-19.
5. Why is the first injection of an mRNA vaccine more harmful than that of a conventional live virus vaccine?
The above argument explains why booster injections will be more toxic with mRNA vaccines, but not why even the first injections of the COVID-19 mRNA vaccines have caused so much more damage than conventional live virus vaccines have done in the past. There are several aspects to this:
- the choice of the antigen—namely, the spike protein, which plays a key role in the pathogenesis of regular COVID-19 disease [6];
- the rapid appearance of the mRNA vaccines in the bloodstream [3], which will lead to the expression of the spike protein in the endothelial cells of the blood vessels, the destruction of these cells by immune attack, and blood clotting;
- the large amount of mRNA contained in each injection. This amount far exceeds the amount of nucleic acids injected with attenuated live vaccines or taken up in case of a natural infection.
We note that only the first stated reason refers to the COVID-19 vaccines specifically. The other two are inherent in the mRNA vaccine technology as such, and they must be expected even with vaccines that encode viral antigens with no intrinsic toxicity. At least the final reason given—namely, the large administered dose of harmful nucleic acid—also applies to the adenovirus-based vaccines produced by Johnson & Johnson and AstraZeneca. However, with these two vaccines, one might hope that the antibody response to the adenoviral proteins of the vector will mitigate the cell destruction caused by booster doses.
6. Conclusion
We have seen that for very general and elementary reasons the mRNA technology is inherently more dangerous than live virus vaccines, which themselves are already less safe than inactivated virus vaccines or subunit vaccines (the latter two varieties were not examined in this paper). Accordingly, the COVID-19 mRNA vaccines should never even have been introduced. Their current application must be stopped, and any further development of this fundamentally flawed vaccine technology should be halted.
Notes
- Even if prior to reinfection antibodies cannot be detected in the bloodstream because the first infection was long ago, we will still have so-called memory B-cells, which can be reactivated on short notice and mount a rapid and forceful antibody response; similarly, memory T-cells exist and can be rapidly activated. Thus, even though the virus will manage to infect a small number of cells, it will have much less time to propagate than it did the first time around—the infection will be snuffed out rapidly, and only an insignificant number of infected cells will have to be killed. This is why we experience childhood diseases only once—immunological memory is ready to spring into action even after decades. Some viruses may manage to multiply even after “neutralization” and uptake into immune cells. In these cases, antibodies tend to make disease worse. This is called antibody-dependent enhancement (ADE) and occurs for example with Dengue virus, but also with coronaviruses, including the causative agent of COVID-19 (SARS-CoV-2).
References
- Goss, J. and Price, M. (2022) Covid-19 Statistics 2022.
- Anonymous, (2021) The Dangers of Booster Shots and COVID-19 `Vaccines’: Boosting Blood Clots and Leaky Vessels.
- Palmer, M. and Bhakdi, S. (2021) The Pfizer mRNA vaccine: Pharmacokinetics and Toxicity.
- Menni, C. et al. (2021) Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: a prospective observational study. Lancet Infect. Dis. 21:939-949
- Parés-Badell, O. et al. (2021) Local and Systemic Adverse Reactions to mRNA COVID-19 Vaccines Comparing Two Vaccine Types and Occurrence of Previous COVID-19 Infection. Vaccines 9 (preprint)
- Marik, P.E. et al. (2021) A scoping review of the pathophysiology of COVID-19. Int. J. Immunopathol. Pharmacol. 35:20587384211048026